Lyme disease in humans is caused by three species of Borrelia bacteria. In North America, Lyme disease is caused primarily by Borrelia burgdorferi, while in Europe the disease is caused mainly by B. garnii and B. afzelli. In Ontario, transmission occurs through the bite of infected blacklegged ticks called Ixodes Scapularis or deer ticks.
The overall risk of acquiring Lyme disease in Toronto is low but is increased if doing activities in wooded and brushy areas.
Note: The City of Toronto has a prevalence of ticks infected with Borrelia burgdorferi greater than 20 per cent and therefore meets the criteria for consideration of post-exposure prophylaxis.
Signs and symptoms usually occur one to two weeks after a tick bite but can begin as early as three days to as long as four weeks after a tick bite.
Lyme borreliosis is generally divided into three stages in which infected persons may experience any of the following symptoms:
Early Localized Disease
Early Disseminated Disease
Late Disease
Erythema migrans (EM) or bull’s eye rash (see below) at the site of a recent tick bite
Fever
Malaise
Headache
Myalgia
Neck stiffness
Fatigue
Arthralgia
Multiple EM in approximately 15 per cent of people occurs several weeks after infective tick bite
Cranial nerve palsies
Lymphocytic meningitis
Conjunctivitis
Arthralgia
Myalgia
Headache
Fatigue
Carditis
May develop in people with early infection that was undetected or not adequately treated. May involve the following:
Heart
Nervous system and joints
Arrhythmias, heart block and sometimes myopericarditis
Recurrent arthritis affecting large joints (i.e., knees)
Peripheral neuropathy
Central nervous system manifestations – meningitis; encephalopathy (i.e., behaviour changes, sleep disturbance, headaches)
Fatigue
Erythemas Migrans
EM represents a response to the bacterium as it spreads intradermally from the site of the tick bite and occurs in 70 to 80 percent of infected persons. Characteristics include:
Occurs within three to 30 days (average seven days) at the bite site; can persist for up to eight weeks.
The rash gradually expands and can reach up to 30 cm across its largest diameter. As it expands, area of the rash may clear resulting in a bull’s-eye appearance.
In many cases, an erythema migrans rash will not present with a classic bull’s-eye appearance.
Rash is rarely itchy or painful; usually feels warm to the touch.
Additional images of typical and atypical rashes are available on Health Canada’s website; under “Clinical manifestations,” please see “Erythema migrans rash.” Note: People with darker skin tones may present with a bruise-like rash.
A skin rash called erythema migrans can develop into a bull’s eye at the site of a tick bite. It is shown here on the upper arm. (Image adapted with permission from Dr. Aucott, John Hopkins Medicine)
Multiple erythema migrans lesions taking variable shapes. (Image adapted with permission from Dr. Aucott, John Hopkins Medicine)
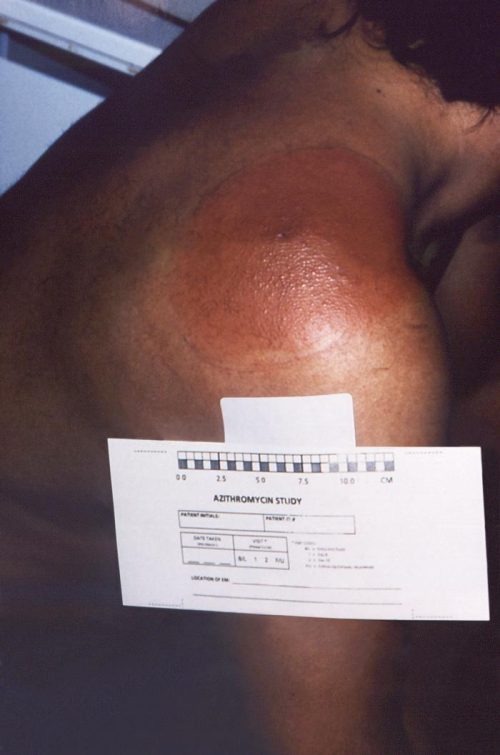
An erythema migrans rash on right shoulder. (Image from CDC.)
Note: An erythematous skin lesion that presents while a tick is still attached or which develops within 48 hours of detachment is most likely a hypersensitivity rather than EM.
Tick bite hypersensitivity is typically less than five cm in largest diameter, has urticarial appearance and begins to disappear within 24 to 48 hours.
There is usually little pain, swelling, itchiness, scaling, exudation or crusting, erosion or ulceration.
Inflammation at the centre of the lesion may or may not be present.
Disease Transmission
In Ontario, blacklegged ticks are the only type of tick that transmits the bacteria that causes Lyme disease.
The risk of human infection increases with the time a tick is attached to a person and usually requires the tick to be attached for 24 hours or more.
Knowledge of a patient’s exposure to Lyme disease risk areas is an important parameter for Lyme disease diagnosis.
Tick populations continue to expand and it is possible that Lyme disease can be acquired outside the currently identified areas.
Ticks can travel or migrate on the bodies of animals such as birds, and therefore can be sporadically present in very low numbers over an even broader area.
Diagnosis, particularly the early stage, is based primarily on clinical symptoms and epidemiological risk factors.
The first step involves testing using a Tier 1 ELISA .
If initial ELISA result is non-reactive, healthcare providers should consider an alternative diagnosis or submit a follow-up specimen (2 – 4 weeks apart) if clinically indicated.
If the initial ELISA result is reactive or indeterminate, sample is further tested using Tier 2 ELISA assay
Blood tests may be negative in patients with early-stage Lyme disease or in patients with early disease who were treated with antibiotics.
The stage of infection and the possible impact of treatment on the outcomes of blood testing should be taken into consideration during diagnosis.
The sensitivity of blood tests increases as the infection progresses
If a patient was exposed to other species of Borrelia such as those that occur in Europe:
Provide travel history and request testing for European Lyme disease.
The specimens from these patients are sent to the National Microbiology Laboratory for antibody testing.
Note: The City of Toronto has a prevalence of ticks infected with Borrelia burgdorferi greater than 20 per cent and therefore meets the criteria for consideration of post-exposure prophylaxis.
A single dose of oral doxycycline may be offered to patients of any age when the following conditions are met:
Adult or nymph of I. scapularis tick was attached for more than 24 hours; and
Prophylaxis can be started within 72 hours from the time that the tick was removed: and
Person was exposed in an area where ecologic information indicates that the rate of infection of ticks is greater than 20 per cent. This applies to the City of Toronto, and
Doxycycline treatment is not contraindicated
There is effective antibiotic treatment for early localized Lyme disease. Should prophylaxis not be indicated based on the above criteria, the health care provider should watch for signs and symptoms of Lyme disease and treat early.
Approximately 10 to 20 per cent of patients may experience persistent or recurrent symptoms following appropriate antibiotic treatment, and are considered to have Post-treatment Lyme Disease Syndrome.